Mike Mandelbaum and Jo Davies from ASIF attended the EULAR PARE 2023 Conference in Brussels on 16 and 17 November. This year’s conference was mostly about implementing the EULAR Manifesto Campaign, an advocacy campaign outlining RMD-related policy asks. The manifesto focuses on influencing three policy areas:
Quality of care: improving RMD prevention, early diagnosis, treatment, and rehabilitation interventions.
Mike presenting the ASIF poster
Social Policy: mitigating the burden of RMDs on health-related quality of life, education, and employment.
Research and innovation: developing better RMD prevention and treatment strategies.
The campaign is largely focussed right now on influencing European Parliament. However, the manifesto will have resonance with all of us and it is a document that could be adapted to suit other countries.
Everyone who attended EULAR PARE also took part in the Best Practice Fair. Forty posters were presented; Mike presented an ASIF poster on IMAS (pictured above). It was wonderful to see the work that other organisations are doing. There were a number of ASIF members at the event.
ASIF has recently gained six new members from Aruba, Brazil, Montenegro, Pakistan, Panama and The Netherlands. We are delighted to introduce Gruparj Petrópolis Institute from Brazil and Arthritis Care Foundation from Pakistan below.
Gruparj Petrópolis Institute, Brazil
Written by Wanda Heloisa Ferreira
“Gruparj Petrópolis Institute completes 22 years of fulfilling its mission: to educate and mobilise society towards the importance of prevention, diagnosis, treatment and early rehabilitation of rheumatic diseases, through health education.”
The Arthritic Patients Group of Rio de Janeiro in Petrópolis – Instituto Gruparj Petrópolis was founded in 2001 with the support of the Rheumatology Society of Rio de Janeiro. In 199 the society held the first Forum for Laymen on Rheumatism in Rio de Janeiro. At the time, rheumatologists observed the population’s lack of knowledge about rheumatic diseases. Since then, Gruparj has worked to meet the needs and interests of people with rheumatic diseases, especially Rheumatoid Arthritis and Spondyloarthritis.
The purpose of the institution is to promote social assistance through information, education and support for people with rheumatic and related diseases; enable and rehabilitate people with functional limitations for the job market; promote patient integration into society; and offer multidisciplinary care to people with rheumatic diseases.
Achievements in Numbers
These numbers are not just statistics; they are tangible testimonies of our positive impact and ongoing commitment to a future with a higher quality of life for people with rheumatic diseases.
2,100 members: A solid community that continues to grow, strengthening connections and collaborations.
10 thousand services per year: Commitment to support, resources and opportunities for our community.
30 thousand people reached: Extending our influence beyond borders, serving not only members, but the community in general.
53 Health Education Courses on Rheumatic Diseases carried out: providing knowledge about treatment, specificities of rheumatic diseases and quality of life for people with rheumatic pathologies across the country.
Comprehensive and Interdisciplinary Service
What makes Instituto Gruparj Petrópolis truly special are its comprehensive activities and services, designed to optimise the physical, emotional and social rehabilitation of people with rheumatic diseases. Our main activities are: lectures, congresses, occupational rehabilitation workshops including through painting and crafts, medical and psychological care and rehabilitation. To achieve this, we count on the effective collaboration of doctors, physiotherapists, occupational and body therapists, psychologists, nutritionists, art therapists, who develop interdisciplinary work, taking into account programming that optimises the physical, emotional and social rehabilitation of people with rheumatic diseases.
Comprehensive and Innovative Support
Multidisciplinary service
Patients meditating
Instituto Gruparj offers medical, psychological, physiotherapeutic, nutritional care, among others, aiming to optimise the physical, emotional and social rehabilitation of patients.
Therapeutic Support – Weekly consultations with a rheumatologist and nutritionist.
Physiotherapy Support – Highlight is the stretching services, offering not only targeted exercises, but also a recreational moment for patients.
Psychological Support – A fundament
al pillar, with group and individual services.
Rehabilitation through Art: Art and Life Project – The project uses art as a means of physical, emotional and social rehabilitation, with weekly workshops.
Educational Events and Awareness Campaigns
The Institute promotes educational events such as lectures, congresses and occupational rehabilitation workshops through art, such as painting and crafts.
A highlight is the Social Medical Meeting on Rheumatic Diseases, bringing together approximately 450 participants annually. In addition, 53 Health Education courses have already been held in Brazil and Portugal.
Awareness campaigns
The social responsibility of Instituto Gruparj Petrópolis is evident in its annual awareness campaigns, open to the community. Annually, the Institute promotes campaigns open to the community on Hepatitis, Osteoporosis, Rheumatoid Arthritis, Lupus, Psoriatic Arthritis and Ankylosing Spondylitis, among others.
Financial Strategy
The institution remains resilient through financial strategies, mobilising resources and seeking support from foundations, companies, the public sector, individual donors, donation campaigns and events, as well as participation in public notices.
In its 22-year journey, the Gruparj Petrópolis Institute has fulfilled its mission, and exceeded expectations, becoming an institution that promotes hope and support for those facing rheumatic diseases. Its trajectory is an inspiration to everyone, highlighting that, with commitment and innovation, we can truly transform lives and communities.
Arthritis Care Foundation (ACF) became a registered trust in 2010 for the welfare of patients with rheumatic diseases in Pakistan. It is the only non-for-profit organisation in Pakistan, striving to provide free and subsidised treatment to less privileged patients from all walks of life. In 2010, three founding members started volunteer services. As of today, eight volunteer rheumatologists and twelve doctors on ACF’s payroll provide services at ACF Centre and five collaborative projects.
Patients’ Care: ACF provides medications (including biologics), diagnostic support and joint replacements for indigent arthritis patients. Apart from patient care, supporting rheumatology fellowship training programmes and arranging awareness seminars are our main objectives. Since inception, PKR 382 million (USD 2.3 million) has been spent on providing free and subsidised treatment to thousands of arthritis patients.
Prof. Nighat Mir examining a patient who lives with rheumatoid arthritis
Each year ACF spends approximately PKR 17,500,000 (USD 61,000) and PKR 20,000,000 (USD 72,500) on provision of biologics and JAK-inhibitor drugs respectively; a significant portion of which is being used for treatment of SpA patients and SLE patients.
In a less developed country like Pakistan, the cost of treating rheumatic diseases is very high, there is little support from the public sector and no health insurance facilities. The Sehat Sahulat Card scheme, recently launched by the government, covers outpatient treatment but does not support full treatment, which leads to many patients suffering poor outcomes and delayed diagnostics.
Teaching and Training: Despite international standards recommending at least 2500 rheumatologists for a population of more than 240 million, Pakistan only has 125 qualified registered rheumatologists. To meet the dire need of specialists, ACF started scholarship support for teaching and training programmes in collaboration with various teaching institutions.
So far 31 rheumatologists have been trained by the ACF Faculty, covering more than 50% of total practising rheumatologists in Punjab province of 120 million. Out of these, 21 specialists have fully or partially been trained through the ACF scholarship programme. ACF funded rheumatologists are not only working in the public and private sector of Pakistan but they are also serving abroad (UK and Middle East). So far around PKR 42 million (USD 2.39 million) has been spent on a scholarship programme for fellows undergoing training.
Education and Research Activities: ACF is consolidating its research endeavours in collaboration with renowned national and international teaching and research institutions. Partnering with the Fatima Jinnah Medical University (FJMU) and National Institute of Health (NIH) USA, ACF is conducting research involving the genetics of lupus in patients and their families. ACF faculty recently conducted research on prevalence of musculoskeletal disorders through a grant by WHO. The ACF team also organised a nine months educational programme for family physicians, covering rigorous modules, with the help of ILAR funding. ACF has set up a support group for ankylosing spondylitis and lupus patients (pictured). Expert rheumatologists and psychologists provided their expert opinions to all registered patients and families in the support group.
Advocacy programmes: ACF team has been actively involved in raising awareness among the general public, physicians and medical students through educational seminars, walks, interviews and public relationship activities. This is part of the ACF commitment towards public awareness about these diseases.
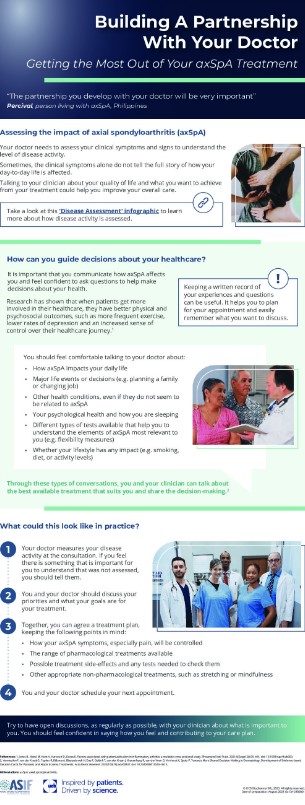
“The partnership you develop with your doctor will be very important” – Percival, person living with axSpA in the Philippines
Building a partnership with a doctor can help people get the most out of their axSpA treatment.
A new ASIF infographic highlights how people living with axSpA can help to guide decisions about their healthcare and what that can look like in practice.
This is part of a series of three infographics to support people living with axSpA better understand how their disease is assessed and how they can make the most of consultations with their doctor.
ASIF’s members are encouraged to share the infographics with their axSpA communities
If you would like a translation of them, please contact Jo Lowe.
The first two infographics are available on our resources pages here.
This series of infographics is a collaboration between ASIF and UCB.
It is becoming clearer that depression and anxiety are prominent among people living with axSpA
The European Map of Axial Spondyloarthritis (EMAS) and the International Map of Axial Spondyloarthritis (IMAS) describe how people living with axSpA experience their disease physically, psychologically and socially. Results show long diagnostic delays and a substantial physical and psychological burden, indicating important unmet needs for patients. Furthermore, axSpA can restrict their ability to participate in their daily routine and lead a productive work life. Understanding the patient’s perspective can improve both health outcomes and enhance shared decision-making between patients and rheumatologists.
The two most common comorbidities of axSpA are hypertension and depression. According to research, patients who exhibit symptoms in the depression-anxiety cluster and/or fibromyalgia-IBS cluster report poorer health and increased axSpA severity. Sleep disorders, anxiety and depression are common among patients and is associated with higher disease activity and functional impairment. But one more question arises when looking at the interconnection between the two. Does depression also impact treatment outcomes? Can there be a connection between treatment and depressive symptoms? And to what extent?
US patients with axSpA in the IMAS study, reported psychological distress and impaired function. Those participants also reported delays in diagnosis – with most of the delays reported by women. It is becoming clearer that depression and anxiety are prominent among people living with axSpA. This is why healthcare professionals should be screening for them in addition to disease activity, level and localisation of pain.
Chronic diseases can impact personal relationships
It is likely that chronic disease with such a broad impact on daily living would also impact interpersonal relationships. Partners are often a main source of support, and they can also be affected by the chronic disease and experience emotional distress themselves. The impact of axSpA on partner relationships is yet to be further researched. A UK study used telephone interviews from people cohabiting with their partner who lives with axSpA. The findings illustrated how living with the disease can influence closeness between partners and dominate daily decisions, particularly surrounding leisure activities. Partners commonly adopted a carer-type role, despite many individuals with axSpA expressing desire for a greater sense of autonomy. This was a unique insight into the lived experiences of both individuals with axSpA and their partners. Findings highlighted the social context of managing a long-term condition and suggested the need for including partners within consultations, and the need for support provision for partners.
Sexual quality of life may be considered a topic lower in the research priorities or in a patient’s life concerns. But this is not the case. There is an ongoing discussion about the relationship between demographics, disease-related variables, treatment, and sexual quality of life (SQOL) in men and women with axSpA. Data suggest that inflammation in patients with axSpA, even in the biologic treatment era, reduces sexual quality of life. On a more specific aspect of sexual quality of life, researchers explored the impact of ankylosing spondylitis (AS) on the sexual relationships of a large cohort of patients across the UK on a total of 1000 patients. They found that AS has a substantial impact on patients’ sexual relationships. One significant finding was that management of AS and its impact on sexual relationships should be directed not only towards physical outcomes such as disease activity and physical function, but also take into consideration the psychological state of the patient.
While reading about the psychological burden of axSpA on the daily lives of patients one can see the link between disease activity, and/or severity, functional limitations, and the presence of mental health issues. The underlying mechanism of disease activity includes chronic pain which cannot be overlooked when discussing the burden of this disease.
Chronic pain leads to a vicious cycle where dysfunctional cognitive schemas (thoughts, core beliefs) and behaviours (attitudes) are used to manage and deal with pain in the activities of daily living (ADL). The basic barriers of managing chronic pain are catastrophizing and fear/avoidance behaviours. When a patient is catastrophizing, basically focusing on thoughts and/or reactions that ‘magnify’ the experience of pain there is an increased likelihood of experiencing depressive and/or anxiety symptoms, greater functional difficulty, or disability. In those cases, patients experience lower quality of life, lower levels of perceived control over pain, lower emotional and social functioning, and poorer response to pharmacological treatments. All these make pain management more difficult. Catastrophizing precedes fear and avoidance behaviours towards pain. In this state, patients are faced with a fear of further injury or the possibility of worsening the medical condition, an increased sense (self-report) of pain and disability, and tend to adopt passive or avoidant strategies and behaviours towards pain.
Interventions
Some well-known interventions to manage the psychological burden of axSpA are Cognitive Behavioural Therapy (CBT) that targets dysfunctional thoughts and behaviours towards pain and functional limitations. Acceptance and Commitment Therapy (ACT) is based on the psychological flexibility model and focuses on acceptance of pain and disability and all related thoughts. Operant-Behavioural Therapy focuses on eliminating dysfunctional behaviours and adopting adaptive responses to pain and disability. Changes occur through the reinforcement (positive or negative) of the links between the ‘threat’ of pain and the physical response
Another intervention is mindfulness-based stress reduction that focuses on teaching self-management through meditation and the practice of daily mindfulness. This aims to increase the patient’s awareness of their body state (e.g. muscle tone, breathing) and, at the same time, develop mindfulness activities. These are some of the available interventions focused on helping patients to be more self-aware and empowered to manage their disease and the burden of it on the activities of their daily living.
Patient organisations can play a vital role in providing support to people living with axSpA
Many patient organisations focus on the empowerment of patients, education and support. This is outlined in the European Patient’s Forum Value of Patient Organisations where it’s stated that “the role patient organisations play in the area of peer support consists of providing knowledge, sharing experiences, and offering emotional, social or practical help to individual patients. It can take several forms such as mentoring, counselling or listening.”
Α feasibility study for developing, implementing and evaluating a peer support intervention for people who were newly diagnosed with early inflammatory arthritis (EIA) showed that early peer support was feasible and well received by both mentors and mentees. In another project, called the iPeer2Peer Program showed that peer support can positively influence the patients’ experiences with a chronic disease. Counselling, peer support and mentorship are important services that patient organisations can provide to their members. Support to members can vary from one organisation to another and from one country to another.
Best practices can be shared and resources and experience from organisations which have already implemented peer support and counselling is of high importance. Psychological support through face-to-face interactions, via group sessions or by using social media platforms should always follow guidelines and be delivered by trained professionals and/or supervised volunteers. Mentors or peer counsellors are often impactful for patients living with a chronic disease given that they can share words of encouragement and support with the unique perspective of the lived experience. In principle, organisations that do not already have experience with offering such support to their members can always network with others that do and share and exchange knowledge and best practices.
Patients living with axSpA manage the difficult realities of a chronic disease, the impact of the diagnostic delays, and medication and treatments, as well as the psychological burden of the disease. Patient organisations can play a vital role in providing support to people living with axSpA.
Nadia Maliou is a MSc Cognitive Psychologist, Vice President of the Hellenic League Against Rheumatism ELEANA, Vice President of the Federation Rare Diseases Greece and a Board Member of Pain Alliance Europe.
Berg, K. H., Rohde, G. E., Prøven, A., Benestad, E. E. P., Østensen, M., & Haugeberg, G. (2019). Sexual quality of life in patients with axial spondyloarthritis in the biologic treatment era. Journal of Rheumatology, 46(9), 1075–1083. https://doi.org/10.3899/jrheum.180413
Garrido-Cumbrera, M., Gálvez-Ruiz, D., Delgado-Domínguez, C. J., Poddubnyy, D., Navarro-Compán, V., Christen, L., … Bundy, C. (2021). Impact of axial spondyloarthritis on mental health in Europe: Results from the EMAS study. RMD Open, 7(3), 1–7. https://doi.org/10.1136/rmdopen-2021-001769
Garrido-Cumbrera, M., Navarro-Compán, V., Webb, D., Jacklin, C., Irwin, S., Christen, L., … Marzo-Ortega, H. (2021). P075 Evaluation of the impact of the COVID-19 pandemic on patients with rheumatic diseases in the UK: results from the REUMAVID study. Rheumatology, 60(Supplement_1), 1–9. https://doi.org/10.1093/rheumatology/keab247.073
Healey, E. L., Haywood, K. L., Jordan, K. P., Garratt, A. M., Ryan, S., & Packham, J. C. (2009). Ankylosing spondylitis and its impact on sexual relationships. Rheumatology (Oxford, England), 48(11), 1378–1381. https://doi.org/10.1093/rheumatology/kep143
Lynch, M. E., Campbell, F., Clark, A. J., Dunbar, M. J., Goldstein, D., Peng, P., … Tupper, H. (2008). A systematic review of the effect of waiting for treatment for chronic pain. Pain, 136(1–2), 97–116. https://doi.org/10.1016/j.pain.2007.06.018
Magrey, M., Walsh, J. A., Flierl, S., Howard, R. A., Calheiros, R. C., Wei, D., & Khan, M. A. (2023). The International Map of Axial Spondyloarthritis Survey: A US Patient Perspective on Diagnosis and Burden of Disease. ACR Open Rheumatology, 5(5), 264–276. https://doi.org/10.1002/acr2.11543
Martindale, J., Shukla, R., & Goodacre, J. (2015). The impact of ankylosing spondylitis/axial spondyloarthritis on work productivity. Best Practice and Research: Clinical Rheumatology, 29(3), 512–523. https://doi.org/10.1016/j.berh.2015.04.002
Otón, T., Sastre, C., & Carmona, L. (2021). The journey of the non-radiographic axial spondyloarthritis patient: the perspective of professionals and patients. Clinical Rheumatology, 40(2), 591–600. https://doi.org/10.1007/s10067-020-05269-z
Raybone, K., Family, H., Sengupta, R., & Jordan, A. (2019). (Un)Spoken realities of living with axial spondyloarthritis:A qualitative study focused on couple experiences. BMJ Open, 9(7), 1–8. https://doi.org/10.1136/bmjopen-2018-025261
Reddy, K. N., Sabu, N., Pandey, N., Raut, A., Joag, K., & Patil, P. (2022). Anxiety and depression among patients with axial spondyloarthritis. Anatolian Journal of Cardiology, 9(1), 8–13. https://doi.org/10.5152/eurjrheum.2021.21022
Roditi, D., & Robinson, M. E. (2011). The role of psychological interventions in the management of patients with chronic pain. Psychology Research and Behavior Management, 4, 41–49. https://doi.org/10.2147/PRBM.S15375
Sandhu, S., Veinot, P., Embuldeniya, G., Brooks, S., Sale, J., Huang, S., … Bell, M. J. (2013). Peer-to-peer mentoring for individuals with early inflammatory arthritis: Feasibility pilot. BMJ Open, 3(3), 1–9. https://doi.org/10.1136/bmjopen-2012-002267
Slouma, M., Bouzid, S., Kharrat, L., Tezeghdenti, A., Ghazouani, E., Metoui, L., … Louzir, B. (2023). Ab0995 Assessment of Matrix Metalloproteinase-3 in Spondyloarthritis: Correlation With Disease Activity. Annals of the Rheumatic Diseases, 82(Suppl 1), 1718.2-1719. https://doi.org/10.1136/annrheumdis-2023-eular.5633
Sturgeon, J. A. (2014). Psychological therapies for the management of chronic pain. Psychology Research and Behavior Management, 7, 115–124. https://doi.org/10.2147/PRBM.S44762
Veehof, M. M., Oskam, M. J., Schreurs, K. M. G., & Bohlmeijer, E. T. (2011). Acceptance-based interventions for the treatment of chronic pain: A systematic review and meta-analysis. Pain, 152(3), 533–542. https://doi.org/10.1016/j.pain.2010.11.002
Wilson, N., Liu, J., Adamjee, Q., Di Giorgio, S., & Lempp, H. (2022). P250 The emotional impact of axial spondyloarthritis: a systematic review and thematic synthesis of qualitative studies and a review of online fora. Rheumatology, 61, Suppl 1, keac133.249. https://doi.org/10.1093/rheumatology/keac133.249
Zhao, P., Yoo, I., Lancey, R., & Varghese, E. (2019). Mobile applications for pain management: An app analysis for clinical usage. BMC Medical Informatics and Decision Making, 19(1), 1–10. https://doi.org/10.1186/s12911-019-0827-7
Zhao, S. S., Radner, H., Siebert, S., Duffield, S. J., Thong, D., Hughes, D. M., … Goodson, N. J. (2019). Comorbidity burden in axial spondyloarthritis: A cluster analysis. Rheumatology (United Kingdom), 58(10), 1746–1754. https://doi.org/10.1093/rheumatology/kez119
Our new Delay to Diagnosis materials will help raise awareness of the key signs and symptoms of axSpA; and the devastating effects of the diagnostic delay.
Three powerful short films, translated into nine languages, and an infographic on the diagnostic delay, including the physical, psychological and socio-economic impacts, will support our members in their advocacy and awareness raising efforts.
These materials are available in a toolkit alongside key messages and suggestions for social media content. The resources have not been designed for a specific timescale or timed campaign and so can be used at any time.
On 12 September 2023ASIF will host two webinars to introduce the materials to our members. To register for the webinar, please email Jo Lowe.
The three main videos will be available on our website on September 12th and Jo will be able to give access to the full toolkits in different languages on request.
Thank you to Dr Raj Sengupta for providing his expert opinion, and to Tseleng, Zhivko, Percival and Jo for their honesty and openness in sharing their personal experiences in these compelling videos.
Rheumatologists from Aruba to Argentina, Pakistan to Panama and so many countries in between spoke to the ASIF team about our work and the impact Patient Organisations make to the lives of people living with axSpA.
During EULAR, some of the world’s leading researchers and rheumatologists discussed the importance of patient centric research and care. We explored our priorities with our industry partners and how, by strengthening our relationships, we can develop projects that our members can use to change lives.
We will share a report on EULAR soon.
AiArthritis’ Go With Us to EULAR 2023 Live Debrief
Saturday, Jun 17, 2023 on Facebook at 12:00 pm EST / 9:00 am PST (USA).
Click here to attend the debrief live or find out how to watch it on demand.
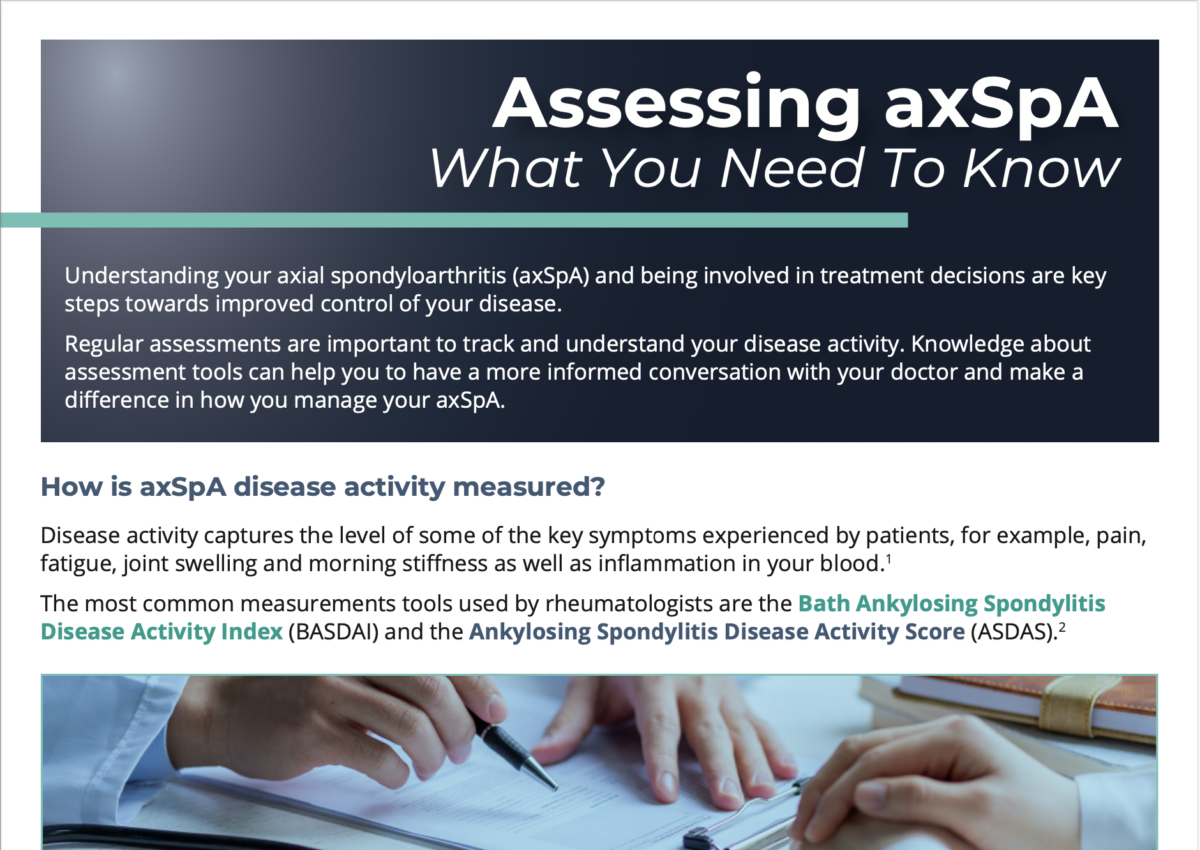
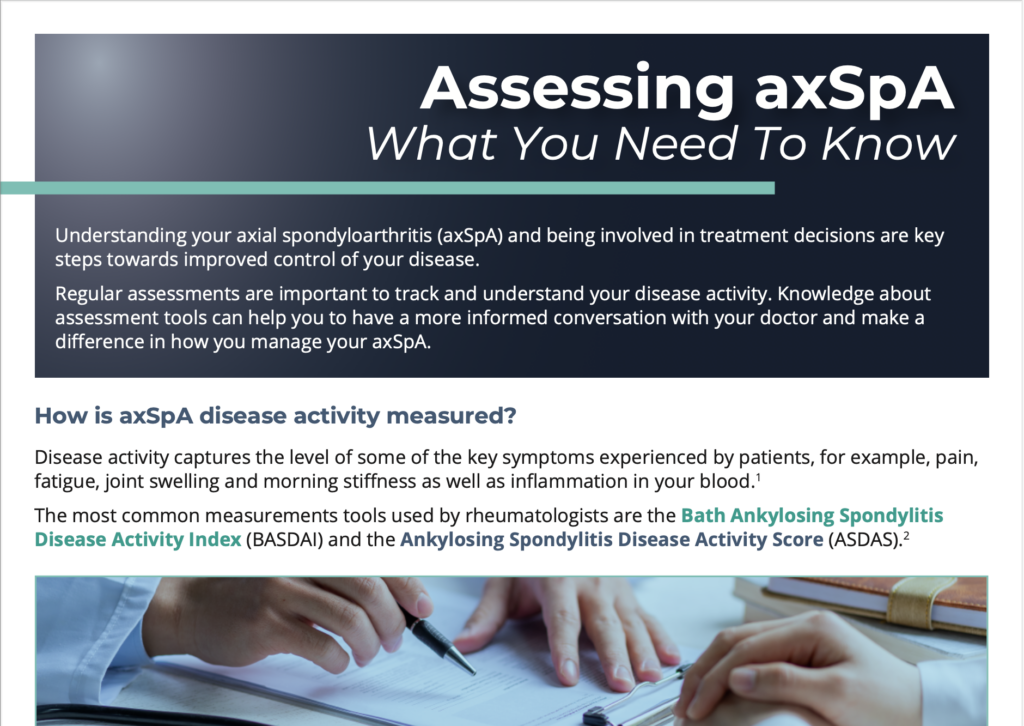
The first in a set of infographics, aimed at preparing and supporting people for appointments with their doctors, is available on our website.
It explains how disease activity is measured, particularly through the BASDAI and ASDAS, as well as other assessments that may be done.
Future infographics will focus on what types of treatment targets are important to patients and addressing barriers to shared decision making. Please let us know if you would like the infographic translated.
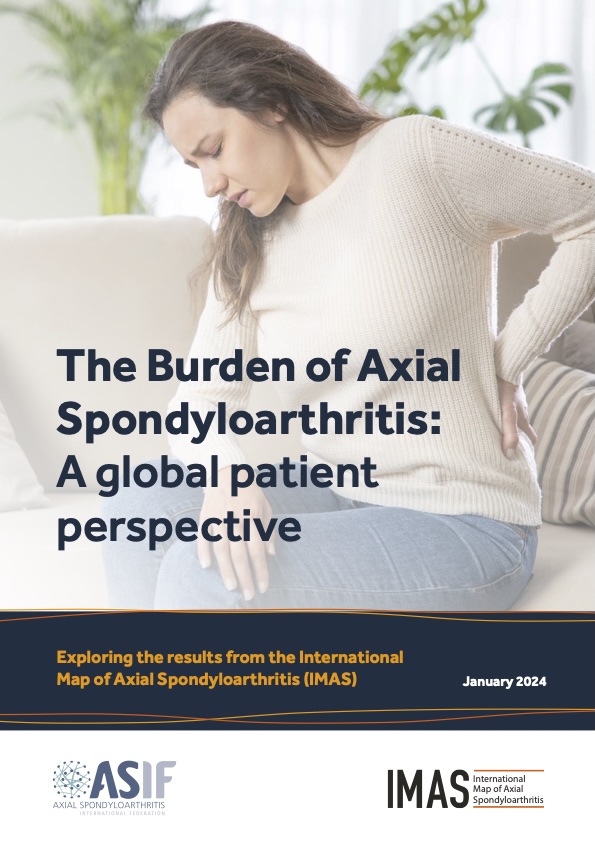
Next month ASIF will launch its International Map of Axial Spondyloarthritis (IMAS) report, The burden of axial spondyloarthritis: a global patient perspective. The report demonstrates the challenges of living with axSpA – from getting a timely diagnosis to the health and socioeconomic impacts. A core aim of IMAS is to incorporate the patient perspective and experience into healthcare policy and into decisions about axSpA care. To support this, the report contains calls to action, aimed at healthcare professionals and policymakers. These include ensuring the needs of axSpA patients are fully understood, that a multidisciplinary approach is taken to care and that healthcare professionals are better equipped to recognise the signs and symptoms of axSpA.
The report will be an invaluable advocacy tool for our members and is an essential read for anyone interested in the impact of axSpA. Using IMAS results, we underline the real-life burden of axSpA on both an individual’s life, and on healthcare utilisation.
In the lead up to the publication of the Report, ASIF continues to spread the word about the reality of living with the disease. Our abstract and presentation at this year’s EULAR congress demonstrated how axSpA can affect almost every area of a person’s life and highlighted numerous unmet needs of those living with the disease.
In November, we presented a poster on the IMAS findings and forthcoming global report at the Galapagos Patient Partnership Day and the EULAR PARE Best Practice Fair. Both events gave ASIF the opportunity to share the IMAS project with other patient organisations and to demonstrate how we can use the evidence gathered through IMAS to advocate for change.
We will continue to disseminate the important results from IMAS; we are busy working with the IMAS scientific committee to prepare five new IMAS abstracts for submission to EULAR 2024.
To coincide with the report publication, new webpages highlighting IMAS’ key findings will be published on the ASIF website, providing a fascinating deep dive into the data. Additional materials, including an advocacy toolkit and infographic showing the key IMAS findings, have also been created to support our members’ work. These resources will be available in January.





 “Gruparj Petrópolis Institute completes 22 years of fulfilling its mission: to educate and mobilise society towards the importance of prevention, diagnosis, treatment and early rehabilitation of rheumatic diseases, through health education.”
“Gruparj Petrópolis Institute completes 22 years of fulfilling its mission: to educate and mobilise society towards the importance of prevention, diagnosis, treatment and early rehabilitation of rheumatic diseases, through health education.”