I am delighted that I have the opportunity to communicate with you through the ASIF newsletter and share my thoughts and excitement about my new post as Chair of the EULAR PARE Committee.
I took over the Chairmanship of the Committee in June from my colleague and friend Elsa Mateus, who was then elected as the new EULAR PARE Vice President. Taking this opportunity, I would like to thank Elsa for her support and guidance through the past year that I was Chair Elect, and reassure her that I look forward to a productive year ahead of us. I would also like to extend my deepest gratitude to Dieter Wiek, who has just ended his term as EULAR PARE Vice President, for sharing his wealth of knowledge and experience with me during the past year.
It is an exciting time to chair the EULAR PARE Committee as EULAR entered a new era in 2021 with a new name, now known as the “European Alliance of Associations for Rheumatology”, with new Statutes and a set-up ready to address the future challenges we all face. EULAR is an umbrella organisation encompassing 45 nations, including EULAR PARE member organisations from 36 countries. The mission of EULAR, is to reduce the impact of rheumatic and musculoskeletal diseases (RMDs) on the individual and society and to improve the social position and the quality of life of people with RMDs in Europe.
EULAR comprises five Content Committees to oversee the many activities to fulfil this mission: Quality of Care, Education, Research, Advocacy and the Congress. Patient representatives are involved in these Committees and our voice is strongly represented in all EULAR activities. In addition, we have our own Representation Committee – the EULAR PARE Committee. This is one of the four Representation Committees and communities which are united in EULAR, the others being EMEUNET (the young rheumatologists) the HPRs (Health Professionals in Rheumatology) and Paediatric Rheumatology.
The EULAR PARE Committee organises a variety of activities and events. Currently we are excited to plan the EULAR Annual European Conference of PARE which will be held virtually in November 2021 under the title ‘Challenges of patient organisations in 2021 and beyond and how to cope’. We look forward to “seeing” some of you there!
We hope that you had the opportunity to attend the EULAR 2021 Virtual Congress in June 2021 and enjoyed participating in some of our EULAR PARE sessions highlighting hot topics like family planning and relationships, volunteering or patient participation in research. If you decide to register to the 2022 Congress and join us in Copenhagen, we can assure you there will be a variety of patient related sessions for you to attend. And why not submit an abstract? Check out the new EULAR Congress website; further details will be shared soon: EULAR 2022 – Abstract submission
Another new and exciting activity has been launched this year: the EULAR PARE Podcasts which feature interviews on various topics and can be found on Spotify and iTunes. Make sure that you don’t miss them – they are fun to listen to!
All information regarding the manifold EULAR PARE activities can be found in the section of the EULAR website devoted to EULAR PARE – enjoy reading all about us here. Subscribe to our e-Breakthrough newsletter to stay in touch, and any questions can be addressed to pare@eular.org
I look very much forward to continuing and strengthening our collaboration and exchange with ASIF. We all work towards the same goals and on making the voice of people with RMDs heard.
I will close this piece by saying that I am proud and honoured to be chairing the EULAR PARE Committee for the next two years, but also very grateful to be part of this family of volunteers who, in a team and motivating spirit, work hand in hand for improving the quality of life of the people living with RMDs in Europe. My personal tip to all: voluntary engagement offers you back so much more than you give – so go for it!
ASIF’s Scientific Adviser, Dr Uta Kiltz attended the virtual EULAR Congress in June, 2021 and reported on some of the highlights. Thank you to Dr Kiltz for this report.
EULAR Report
1. Dysbiosis (disruption or imbalance) of the gut microbiota (microorganisms).
Immune-mediated diseases such as spondyloarthritis (SpA) consistently show an imbalance of the gut microbiota and frequently occur with other inflammatory conditions such as Crohn’s disease (CD) and acute anterior uveitis (AAU). In a study, a total of 300 patients were recruited (111 with axial SpA, 110 with anterior acute uveitis, and 79 with Crohn´s Disease) and were compared to 63 control individuals who did not have any of the three conditions. The investigators analyzed microbiota composition in stool samples. The 300 patients showed a shared gut microbiome composition that differed from that of the 63 control individuals. The study authors concluded that the 300 patients with different immune-mediated diseases showed many shared related microorganisms in their gut microbiota and some of these were associated to the presence of HLA-B27. In addition, the individual diseases showed distinct characteristics. All the patients frequently showed fewer or more of certain microorganisms compared to the non-patients. The study showed how looking at gut microbiota may help understand the cause of SpA and its related diseases.
Reference: OP0031 SHARED AND DISTINCT GUT MICROBIOME SIGNATURES IN PATIENTS WITH AXIAL SPONDYLOARTHRITIS AND ITS RELATED IMMUNE-MEDIATED DISEASES by V. Rios Rodriguez et al.
2. Peripheral manifestations in spondyloarthritis
Patients with a diagnosis of Spondyloarthritis (SpA) and Psoriatic Arthritis (PsA) may have mainly axial or peripheral symptoms, and the frequency and distribution of these symptoms may determine the clinical diagnosis by the rheumatologist. For the study, these are called “clinical clusters”, in other words, those symptoms rheumatologists take into consideration to make a diagnosis.
The objective of the study was to identify “statistical clusters” of peripheral involvement according to the specific location of symptoms, and see how statistical clusters compared to clinical clusters. The study was a sub analysis of the worldwide cross-sectional and multicentre ‘PerSpA’ study conducted in 24 participating countries. Four different cluster analyses were conducted: the first one using information about the specific location from all the peripheral musculoskeletal manifestations (i.e., peripheral arthritis, enthesitis and dactylitis), and thereafter a cluster analysis for each peripheral manifestation individually.
4,465 patients were included in the analysis. Two clusters were found with regard to the location of all the peripheral manifestations. Three clusters were found with regard to the location of the peripheral arthritis. Clusters 2 and 3 showed a high prevalence of peripheral joint disease, although this was located more predominantly in the lower limbs in cluster 2, and in the upper limbs in cluster 3. Cluster 1 showed a higher prevalence of males, HLA-B27 positivity, axial involvement, a lower presence of psoriasis, a more frequent diagnosis of axSpA and fulfilling the ASAS axSpA criteria in comparison with clusters 2 and 3, respectively. Clusters 2 and 3 showed a higher prevalence of enthesitis and dactylitis in comparison with cluster 1, a more frequent diagnosis of PsA and fulfillment of the CASPAR criteria.
These results suggest the presence of dissimilar patterns of peripheral involvement in SpA and PsA patients without clearly defined groups, confirming the clear overlap of these peripheral manifestations across the different underlying diagnoses.
Reference: OP0047 IDENTIFICATION OF CLINICAL PHENOTYPES IN PATIENTS WITH AXIAL SPONDYLOARTHRITIS, PERIPHERAL SPONDYLOARTHRITIS AND PSORIATIC ARTHRITIS ACCORDING TO PERIPHERAL MUSCULOSKELETAL MANIFESTATIONS: A CLUSTER ANALYSIS IN THE INTERNATIONAL ASAS-PERSPA STUDY by Lopez Medina et al.
3. Sex differences in patient-reported outcomes
It is well known that female score consistently higher in patient-reported outcomes. However, this does not necessarily correlate to worse clinical findings. A study from Ireland investigated whether scores differ in males and females across the individual components of the BASDAI (Bath Ankylosing Spondylitis Disease Activity Index).
A total of 857 patients were included in the analysis. Within the BASDAI, females scored significantly worse than males across all components. Females recorded highest mean scores for fatigue (5.56), while males recorded highest mean scores for spinal pain (4.63). Lowest mean scores for both genders was for EMS (Early Morning Stiffness) duration (3.54 vs 3.12). Ranking of the BASDAI components by mean scores show similarity in the ranking of discomfort, EMS, other pain and EMS duration.
The authors showed that axSpA females have consistently worse Patient Reported Outcomes but have better spinal mobility than males. Despite females recording worse BASDAI scores than males, the pattern of active disease is similar in 4 of the 6 components of the BASDAI. However, fatigue is the most problematic symptom in females with active axSpA while spinal pain is the most problematic symptom for males. This variation by gender should be kept in mind when evaluating a patient with suspected active axSpA.
Reference: OP0051 LOOKING BEYOND BASDAI TOTAL SCORES: ANALYSIS OF THE BASDAI ON THE BASIS OF SEX by Sinead Maguire
4. How to define refractory disease in axSpA
In clinical practice, some patients with axial spondyloarthritis (axSpA) fail several consecutive biological treatments (bDMARDs). How this group of “refractory” (not responding) patients should best be defined, how common they are, and what their characteristics are, is poorly understood.
Patients with axSpA starting a first bDMARD in 2009-2018 were identified in this observational prospective cohort study. Refractory disease was defined based on the number of different bDMARD treatments started in individual patients: mild (up to 3 bDMARDs), moderate (4), and strict (5 or more). The point prevalence of refractory axSpA increased over time.
Among 12,037 included axSpA patients (64% male), the point-prevalence of bDMARD refractory disease in 2018 was 16%/7%/3% according to mild/moderate/strict definitions. In this large Nordic observational cohort of axSpA patients treated in routine care, it was possible to demonstrate that a substantial proportion of all patients had used multiple bDMARDs. In 2018, one in six patients had received up to 3 bDMARDs, indicating a bDMARD refractory disease. Multiple switching was more frequent during later years, probably due to more bDMARDs becoming available. The characteristics of refractory axSpA, including sex and disease activity, will have to be further explored, as will the impact of refractory disease on long-term outcomes.
Reference: OP0140 BIOLOGIC REFRACTORY DISEASE IN AXIAL SPONDYLOARTHRITIS – DEFINITION, PREVALENCE AND PATIENT CHARACTERISTICS. A COLLABORATION BETWEEN FIVE NORDIC BIOLOGIC REGISTRIES by D. DI Giuseppe et al
5. Work participation in patients with axSpA.
It is well-known that patients with axSpA have impaired or lower work participation. In this study, 787 patients with axSpA were investigated to characterise the different aspects of work participation [presenteeism, absenteeism, sick leave, unemployment, disability pensions] and their associations with demographic and other clinical factors.
Despite improvements in medical treatment options for axSpA, substantial impaired work participation was observed. Patients with impaired work participation compared to patients with no impairment, reported increased fatigue, longer duration of morning stiffness, decreased functional capacity, female sex and a lower level of education.
Reference: POS0983 WORK PARTICIPATION IN PATIENTS WITH AXIAL SPONDYLOARTHRITIS IN GERMANY: RESULTS FROM A MULTICENTER, OBSERVATIONAL SURVEY (ATTENTUS-axSpA) by U. Kiltz et al.
Michael Mallinson, ASIF Volunteer, wrote the following report on the session – thank you Michael
‘Fatigue in Arthritis, SpA and systemic rheumatic diseases’ by Prof. RN Jette Primdahl
The most common complaints of patients with inflammatory arthritis are pain and fatigue, with as many of half of all patients with spondyloarthritis experiencing fatigue. But what is fatigue, what causes it and how can it be dealt with? This was the topic of a session at EULAR 2021 given by Prof. RN Jette Primdahl.
The causes of fatigue are pain intensity rather than inflammation measured by CRP or ESR, poor sleep, depression, worries and anxieties and to some degree, disability. But there are also psycho-social issues with fatigue, such as poor interpersonal relations, perceived social support, perception of illness, feeling helpless or out of control, the patient’s roles and function in everyday life and a low degree of self-efficacy, that is a low belief in oneself to succeed in a particular situation. And lastly, more women than men suffer from fatigue.
Fatigue is a multi-dimensional symptom of disease-related factors as well as personal, behavioural and social factors and cognitive and emotional factors. This means that people living with fatigue experience physical, cognitive, emotional and behavioural impacts. They do not just feel tired and lacking in energy, they also have concentration and memory issues, feelings of frustration and hopelessness, decreased motivation, and a failure to plan and be spontaneous.
And how do patients deal with fatigue? Through taking breaks and relaxing through the day, or taking a day off; by prioritising tasks and by asking for help. And what is there to help patients with fatigue? There are pharmaceutical treatments such as biologics and conventional DMARDS that can reduce inflammation and pain and lead to small to moderate improvements in fatigue. But professional help for depression may be required and the effects of all medications for any co-morbidities needs to be examined to see if any worsen fatigue.
We know that exercise is important for patients with spondyloarthritis and it is no less so to help reduce fatigue. Other non-pharmacological treatments include patient education on self-managing fatigue, pain and sleep; goal setting, problem solving, action planning and communication training; cognitive behavioural therapy and motivational interviewing; activity diaries and guided reflections, and lastly, pacing and prioritizing, particularly for the management of fatigue at work.
What can clinicians do to address fatigue? First, they can ask their patients if they suffer from fatigue and how it affects their lives. Second, they can inform their patients that they are not alone, with between 35% and 85% depending on the condition of patients with inflammatory arthritis reporting fatigue, and offer information on fatigue. Third, they can encourage more physical activity with individually targeted guidance to do so. Fourth, they can look at pharmacological treatments and make any relevant changes. Lastly, they can offer psycho-social support.
In summary, Prof. Primdahl said that there needs to be acknowledgement that fatigue is a major problem for patients with arthritis and spondyloarthritis and more research into its causes. There also needs to be further development and testing of targeted interventions. Most importantly, there needs to be implementation of the evidence of pharmacological and non-pharmacological management of fatigue in clinical practice.
On 7 July, we held our launch events for our new Delay to Diagnosis report. We were delighted to welcome patient organisations, patients, rheumatologists, other healthcare professionals, representatives from the pharmaceutical industry and researchers to the virtual sessions. Attendees from over 20 countries took part in stimulating and valuable live Q&A with our expert panellists. Thank you to everyone who joined us and who contributed to the thought-provoking debates.
We have been overwhelmed by the positive feedback received from around the world. We hope the report is a valuable tool for our members who are advocating for change in their country. Please contact Jo Lowe for support in using the report with stakeholders.
We know this is only the start of a long-term campaign to reduce the international delay to diagnosis. We are working on the next steps and look forward to discussing them with you soon.
We are hugely grateful to Maranda van Dam from South Africa, Annie McPherson from Australia and Kel Arceo from the Philippines for sharing their turmoil whilst waiting for a diagnosis in such an honest and raw way. Their three short films were a highlight of the launch events and have been watched many times on social media and on the website.
Thank you to Raj Mahapatra, ASIF Trustee, for Chairing both launch events, and to our presenters and panellists: Drs Shashank Akerkar, Floris van Gaalen, Dale Webb, Helena Marzo-Ortega, Muhammad Asim Khan and Wilson Bautista-Molano, Annie McPherson, Kel Arceo, Lillann Wermskog, Maranda van Dam and Ricky White, for their unique contribution to the events.
If you would like the report or the patient videos translated, please get in touch.
Ankylosing Spondylitis Group of Australia Queensland presented to rheumatologists, organised a picnic/exercise day on World AS Day and promoted the campaign on social media
AntarDhwani – Ankylosing spondylitis society in Ahmedabad India, launched a book about Ankylosing Spondylitis and held a virtual event for rheumatologists, spine specialists, psychologists, GPs and patients
Association France Spondyloarthrites hosted a Hatha Yoga session and health and emotion coaching session on YouTube
Axial Spondyloarthritis Association of South Africa held a virtual workshop focused on emotional wellbeing
Bulgarian Ankylosing Spondylitis Patient Society translated our WASD materials into Bulgarian
Canadian Spondylitis Association held a number of webinars in support of WASD as well as encouraging participation in Walk Your AS Off
CEADE Coordinadora Española de Asociaciones de Espondiloartritis shared our WASD material on social media
Magyar Bechterewesek Egyesülete, Hungary, released two videos of discussions focused on the importance of movement and the connection between exercise and mental health. The videos can be viewed on their website.
National Axial Spondyloarthritis Society in UK hosted a meeting of the All Parliamentary Group for Axial Spondyloarthritis which focused on mental health.
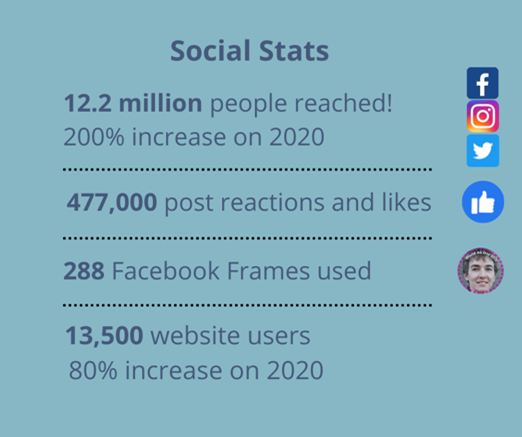
Spafo Norway reached 19,216 people through their social media from March to 8 May.
This project will provide members with an improved and more cohesive set of tools to assist you with fundraising; governance; lobbying and advocacy; communications and social media, as well as setting up a new organisation. These resources will be supplemented with a range of assets, including a new, digital ‘What is axSpA?’ brochure, guidance on various elements of living with axSpA and provide statistical information on different factors related to the disease. All of these assets will be readily available to be translated into other languages.
Having now fully defined the project, we are working with an agency to support us designing and writing the new resources. We look forward to giving further updates and getting your feedback over the coming months.
Please email Jo Lowe with ideas for resources you think would be valuable.
The IMAS survey continues to expand and has now launched in the UK, Philippines and the USA. This provides the opportunity to collect invaluable data from people living with axSpA in these regions. The survey will be launched in Lithuania, South Africa and Argentina by the end of August and India is also expected to launch the survey in the near future.
The first Talk to be Heard video was launched on World AS Day and focused on patients’ experience of axSpA and the effect on their emotional health. As part of the series, three more videos will be released in the coming months. These will focus on the themes of working and living with axSpA; axSpA and relationships; and talking about treatment goals. The ASIF team are working closely with Novartis to create a campaign around these short films that will encourage people to talk about the range of ways axSpA affects their lives – and ultimately support them in talking to their rheumatologist or loved ones.
New webpages, which bring to life the breadth of data from IMAS and powerfully depict the many ways that axSpA affects those living with it, will be published on the ASIF IMAS webpage soon. The new pages will help to communicate the lived reality of axSpA as well as provide a valuable tool for all those lobbying for change.
We currently have 200 registered members that have axSpA.
With a growing membership daily, our role has never been more important.
If we look at the world numbers, and we use a conservative estimate in South Africa of 1 in 500, we would be looking at roughly 160 000 patients with axSpA in South Africa. A lot of patients are not diagnosed or are diagnosed with mechanical back pain without having any treatment.
We have a huge, underdiagnosed situation in our country and if you think about the 80 rheumatologists we have and 60 million strong population, that is little wonder.
This problem spreads into Africa, where there are merely a handful of rheumatologists that service all the countries. Most of the patients are then sent to South Africa for treatment.
Voice of the Expert and Voice of the Patient Campaign
South Africa has been in lockdown for most of 2021. This has caused a great deal of anxiety and stress among our members.
To bridge that, we then aimed to make a connection, bringing the experts to our patients, in the comfort of their own homes.
The Voice of the Patient campaign was designed to bring live witness to patients that have axSpA, to share their own personal story with our members. This also creates the feeling of shared mutual disease burden and makes our patients feel less alone.
The feedback has been overwhelming and this has been the most asked for resource since we have launched this campaign
This has also given our rheumatologists the chance to get involved with the axSpA community.
Walk Your AS Off
South Africa walked this year in full force, and more than doubled our steps to over 7 million. More than 42 members participated in this event.
Walk Your AS Off takes place in May, and is a one of many activities around World AS Day.
– By Maranda van Dam, Chairperson of Axial Spondyloarthritis Association of South Africa
Find out more about the Axial Spondyloarthritis Association of South Africa.