Written by Muhammad A. Khan, MD, FRCP, MACP, Professor Emeritus of Medicine, Case Western Reserve School of Medicine, USA
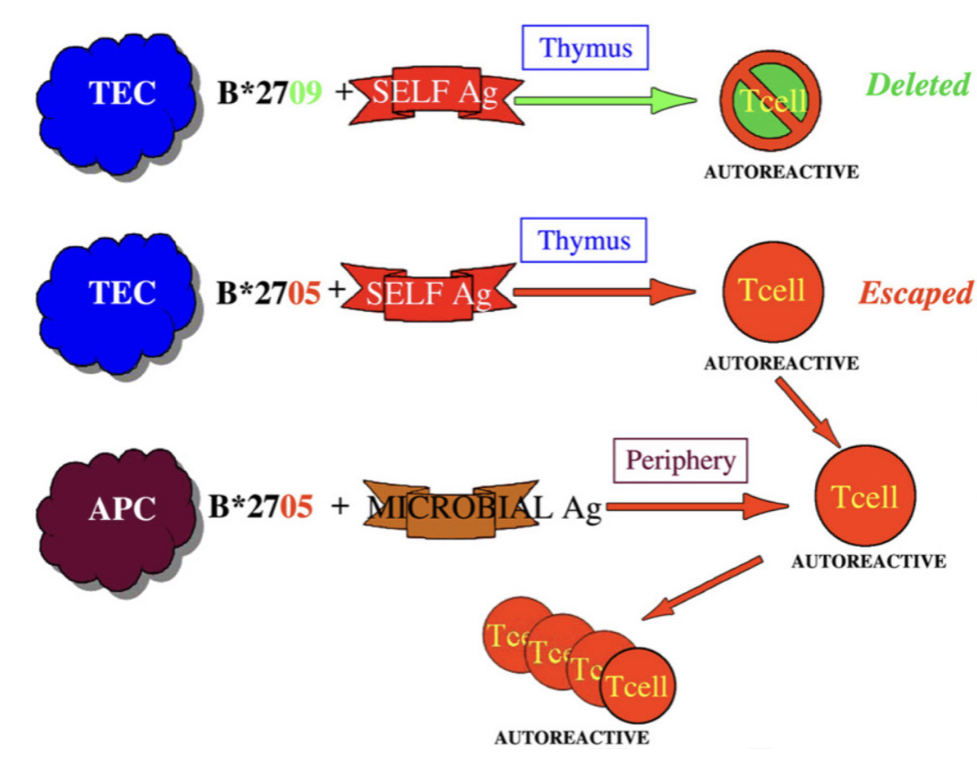
This year marks the 50th anniversary of the groundbreaking discovery linking HLA-B27 to ankylosing spondylitis (AS)[1,2]. Beyond HLA-B27, over 116 additional recognised genetic risk factors have been identified, while exploration of environmental factors in this context remains limited [1,2]. Notably, HLA-B27(+) AS patients exhibit a distinct clone of potentially autoreactive (self-reactive) CD8+ T cells with TRBV9-containing T cell receptors (TCR) in their bloodstream and within inflamed tissues [2-4].
Figure 1 elucidates the persistence of autoreactive CD8+ T cells that manage to evade elimination in the thymus during early life. This phenomenon is observed in individuals born with the disease-predisposing HLA-B27 subtype (HLA-B27:05) but not in those born with the non-disease-predisposing subtype (HLA-B27:09) [3]. The proposed mechanism involves clonal expansion of these T cells upon exposure to microbial-derived peptides, followed by cross-reactivity with self-derived peptides. This cascade triggers an autoimmune inflammatory process, ultimately in AS in individuals with the disease-predisposing subtypes of HLA-B27 [3].
A recent outstanding study from a year ago has effectivelyunravelled the 50-year-old puzzle surrounding HLA-B27’s role in AS [5]. This breakthrough has notably expedited the potential for targeting and eliminating disease-causing T cells, offering promising prospects for curing those affected [5].
A subsequent groundbreaking paper, published a month ago, highlights the success of targeted elimination of the disease-causing TRBV9+ T cells in an HLA-B27(+) patient with AS [6]. After successful testing in nonhuman primate models, the authors observed a dramatic efficacy in elimination of these T cells in AS. The patient achieved remission within 3 months, discontinuing anti-TNF therapy used for 5 years. Complete remission has now persisted for 4 years, with three annual doses of anti-TRBV9 treatment [6].
The authors aptly concluded that the selective depletion of a TRBV9-defined group of T cells presents a promising avenue for safe and effective therapies in AS. This innovative approach may extend to other HLA-B27-associated forms of spondyloarthritis [6]. Targeted elimination of the disease’s root cause, without resorting to systemic immunosuppression, holds the potential for a new era of safe and efficient autoimmune therapies.
These pivotal advancements not only signify a paradigm shift but also enhance the prospect of preventing the disease in individuals with high-genetic risk factors [5,6]. Furthermore, the discovery of enhanced biomarkers, coupled with the evolving technology of electric field molecular fingerprinting, holds promise for significantly improving early diagnosis and facilitating the initiation of curative treatments [2].
REFERENCES:
Braun J, Sieper J. Fifty years after the discovery of the association of HLA B27 with ankylosing spondylitis. RMD Open. 2023 Aug;9(3):e003102. doi: 10.1136/rmdopen-2023-003102.
Khan MA. HLA-B*27 and ankylosing spondylitis: 50 years of insights and discoveries. Curr Rheumatol Rep. 2023. doi: 10.1007/s11926-023-01118-5.
Khan MA, Mathieu A, Sorrentino R, Akkoc N. The pathogenetic role of HLA-B27 and its subtypes. Autoimmun Rev. 2007;6(3):183-9. doi: 10.1016/j.autrev.2006.11.003.
Garrido-Mesa J, Brown MA. T cell Repertoire Profiling and the Mechanism by which HLA-B27 Causes Ankylosing Spondylitis. Curr Rheumatol Rep. 2022 Dec;24(12):398-410. doi: 10.1007/s11926-022-01090-6.
Yang X, Garner LI, Zvyagin IV, Paley MA, Komech EA, Jude KM, et al. Autoimmunity-associated T cell receptors recognize HLA-B*27-bound peptides. Nature. 2022;612(7941):771-7. doi: 10.1038/s41586-022-05501-7.
Britanova OV, Lupyr KR, Staroverov DB, Shagina IA, Somov DV, Klimenko A, et al. Targeted depletion of TRBV9+ T cells as immunotherapy in a patient with ankylosing spondylitis. Nat Med. Oct 23; 2023. doi: 10.1038/s41591-023-02613-z.
It is becoming clearer that depression and anxiety are prominent among people living with axSpA
The European Map of Axial Spondyloarthritis (EMAS) and the International Map of Axial Spondyloarthritis (IMAS) describe how people living with axSpA experience their disease physically, psychologically and socially. Results show long diagnostic delays and a substantial physical and psychological burden, indicating important unmet needs for patients. Furthermore, axSpA can restrict their ability to participate in their daily routine and lead a productive work life. Understanding the patient’s perspective can improve both health outcomes and enhance shared decision-making between patients and rheumatologists.
The two most common comorbidities of axSpA are hypertension and depression. According to research, patients who exhibit symptoms in the depression-anxiety cluster and/or fibromyalgia-IBS cluster report poorer health and increased axSpA severity. Sleep disorders, anxiety and depression are common among patients and is associated with higher disease activity and functional impairment. But one more question arises when looking at the interconnection between the two. Does depression also impact treatment outcomes? Can there be a connection between treatment and depressive symptoms? And to what extent?
US patients with axSpA in the IMAS study, reported psychological distress and impaired function. Those participants also reported delays in diagnosis – with most of the delays reported by women. It is becoming clearer that depression and anxiety are prominent among people living with axSpA. This is why healthcare professionals should be screening for them in addition to disease activity, level and localisation of pain.
Chronic diseases can impact personal relationships
It is likely that chronic disease with such a broad impact on daily living would also impact interpersonal relationships. Partners are often a main source of support, and they can also be affected by the chronic disease and experience emotional distress themselves. The impact of axSpA on partner relationships is yet to be further researched. A UK study used telephone interviews from people cohabiting with their partner who lives with axSpA. The findings illustrated how living with the disease can influence closeness between partners and dominate daily decisions, particularly surrounding leisure activities. Partners commonly adopted a carer-type role, despite many individuals with axSpA expressing desire for a greater sense of autonomy. This was a unique insight into the lived experiences of both individuals with axSpA and their partners. Findings highlighted the social context of managing a long-term condition and suggested the need for including partners within consultations, and the need for support provision for partners.
Sexual quality of life may be considered a topic lower in the research priorities or in a patient’s life concerns. But this is not the case. There is an ongoing discussion about the relationship between demographics, disease-related variables, treatment, and sexual quality of life (SQOL) in men and women with axSpA. Data suggest that inflammation in patients with axSpA, even in the biologic treatment era, reduces sexual quality of life. On a more specific aspect of sexual quality of life, researchers explored the impact of ankylosing spondylitis (AS) on the sexual relationships of a large cohort of patients across the UK on a total of 1000 patients. They found that AS has a substantial impact on patients’ sexual relationships. One significant finding was that management of AS and its impact on sexual relationships should be directed not only towards physical outcomes such as disease activity and physical function, but also take into consideration the psychological state of the patient.
While reading about the psychological burden of axSpA on the daily lives of patients one can see the link between disease activity, and/or severity, functional limitations, and the presence of mental health issues. The underlying mechanism of disease activity includes chronic pain which cannot be overlooked when discussing the burden of this disease.
Chronic pain leads to a vicious cycle where dysfunctional cognitive schemas (thoughts, core beliefs) and behaviours (attitudes) are used to manage and deal with pain in the activities of daily living (ADL). The basic barriers of managing chronic pain are catastrophizing and fear/avoidance behaviours. When a patient is catastrophizing, basically focusing on thoughts and/or reactions that ‘magnify’ the experience of pain there is an increased likelihood of experiencing depressive and/or anxiety symptoms, greater functional difficulty, or disability. In those cases, patients experience lower quality of life, lower levels of perceived control over pain, lower emotional and social functioning, and poorer response to pharmacological treatments. All these make pain management more difficult. Catastrophizing precedes fear and avoidance behaviours towards pain. In this state, patients are faced with a fear of further injury or the possibility of worsening the medical condition, an increased sense (self-report) of pain and disability, and tend to adopt passive or avoidant strategies and behaviours towards pain.
Interventions
Some well-known interventions to manage the psychological burden of axSpA are Cognitive Behavioural Therapy (CBT) that targets dysfunctional thoughts and behaviours towards pain and functional limitations. Acceptance and Commitment Therapy (ACT) is based on the psychological flexibility model and focuses on acceptance of pain and disability and all related thoughts. Operant-Behavioural Therapy focuses on eliminating dysfunctional behaviours and adopting adaptive responses to pain and disability. Changes occur through the reinforcement (positive or negative) of the links between the ‘threat’ of pain and the physical response
Another intervention is mindfulness-based stress reduction that focuses on teaching self-management through meditation and the practice of daily mindfulness. This aims to increase the patient’s awareness of their body state (e.g. muscle tone, breathing) and, at the same time, develop mindfulness activities. These are some of the available interventions focused on helping patients to be more self-aware and empowered to manage their disease and the burden of it on the activities of their daily living.
Patient organisations can play a vital role in providing support to people living with axSpA
Many patient organisations focus on the empowerment of patients, education and support. This is outlined in the European Patient’s Forum Value of Patient Organisations where it’s stated that “the role patient organisations play in the area of peer support consists of providing knowledge, sharing experiences, and offering emotional, social or practical help to individual patients. It can take several forms such as mentoring, counselling or listening.”
Α feasibility study for developing, implementing and evaluating a peer support intervention for people who were newly diagnosed with early inflammatory arthritis (EIA) showed that early peer support was feasible and well received by both mentors and mentees. In another project, called the iPeer2Peer Program showed that peer support can positively influence the patients’ experiences with a chronic disease. Counselling, peer support and mentorship are important services that patient organisations can provide to their members. Support to members can vary from one organisation to another and from one country to another.
Best practices can be shared and resources and experience from organisations which have already implemented peer support and counselling is of high importance. Psychological support through face-to-face interactions, via group sessions or by using social media platforms should always follow guidelines and be delivered by trained professionals and/or supervised volunteers. Mentors or peer counsellors are often impactful for patients living with a chronic disease given that they can share words of encouragement and support with the unique perspective of the lived experience. In principle, organisations that do not already have experience with offering such support to their members can always network with others that do and share and exchange knowledge and best practices.
Patients living with axSpA manage the difficult realities of a chronic disease, the impact of the diagnostic delays, and medication and treatments, as well as the psychological burden of the disease. Patient organisations can play a vital role in providing support to people living with axSpA.
Nadia Maliou is a MSc Cognitive Psychologist, Vice President of the Hellenic League Against Rheumatism ELEANA, Vice President of the Federation Rare Diseases Greece and a Board Member of Pain Alliance Europe.
Berg, K. H., Rohde, G. E., Prøven, A., Benestad, E. E. P., Østensen, M., & Haugeberg, G. (2019). Sexual quality of life in patients with axial spondyloarthritis in the biologic treatment era. Journal of Rheumatology, 46(9), 1075–1083. https://doi.org/10.3899/jrheum.180413
Garrido-Cumbrera, M., Gálvez-Ruiz, D., Delgado-Domínguez, C. J., Poddubnyy, D., Navarro-Compán, V., Christen, L., … Bundy, C. (2021). Impact of axial spondyloarthritis on mental health in Europe: Results from the EMAS study. RMD Open, 7(3), 1–7. https://doi.org/10.1136/rmdopen-2021-001769
Garrido-Cumbrera, M., Navarro-Compán, V., Webb, D., Jacklin, C., Irwin, S., Christen, L., … Marzo-Ortega, H. (2021). P075 Evaluation of the impact of the COVID-19 pandemic on patients with rheumatic diseases in the UK: results from the REUMAVID study. Rheumatology, 60(Supplement_1), 1–9. https://doi.org/10.1093/rheumatology/keab247.073
Healey, E. L., Haywood, K. L., Jordan, K. P., Garratt, A. M., Ryan, S., & Packham, J. C. (2009). Ankylosing spondylitis and its impact on sexual relationships. Rheumatology (Oxford, England), 48(11), 1378–1381. https://doi.org/10.1093/rheumatology/kep143
Lynch, M. E., Campbell, F., Clark, A. J., Dunbar, M. J., Goldstein, D., Peng, P., … Tupper, H. (2008). A systematic review of the effect of waiting for treatment for chronic pain. Pain, 136(1–2), 97–116. https://doi.org/10.1016/j.pain.2007.06.018
Magrey, M., Walsh, J. A., Flierl, S., Howard, R. A., Calheiros, R. C., Wei, D., & Khan, M. A. (2023). The International Map of Axial Spondyloarthritis Survey: A US Patient Perspective on Diagnosis and Burden of Disease. ACR Open Rheumatology, 5(5), 264–276. https://doi.org/10.1002/acr2.11543
Martindale, J., Shukla, R., & Goodacre, J. (2015). The impact of ankylosing spondylitis/axial spondyloarthritis on work productivity. Best Practice and Research: Clinical Rheumatology, 29(3), 512–523. https://doi.org/10.1016/j.berh.2015.04.002
Otón, T., Sastre, C., & Carmona, L. (2021). The journey of the non-radiographic axial spondyloarthritis patient: the perspective of professionals and patients. Clinical Rheumatology, 40(2), 591–600. https://doi.org/10.1007/s10067-020-05269-z
Raybone, K., Family, H., Sengupta, R., & Jordan, A. (2019). (Un)Spoken realities of living with axial spondyloarthritis:A qualitative study focused on couple experiences. BMJ Open, 9(7), 1–8. https://doi.org/10.1136/bmjopen-2018-025261
Reddy, K. N., Sabu, N., Pandey, N., Raut, A., Joag, K., & Patil, P. (2022). Anxiety and depression among patients with axial spondyloarthritis. Anatolian Journal of Cardiology, 9(1), 8–13. https://doi.org/10.5152/eurjrheum.2021.21022
Roditi, D., & Robinson, M. E. (2011). The role of psychological interventions in the management of patients with chronic pain. Psychology Research and Behavior Management, 4, 41–49. https://doi.org/10.2147/PRBM.S15375
Sandhu, S., Veinot, P., Embuldeniya, G., Brooks, S., Sale, J., Huang, S., … Bell, M. J. (2013). Peer-to-peer mentoring for individuals with early inflammatory arthritis: Feasibility pilot. BMJ Open, 3(3), 1–9. https://doi.org/10.1136/bmjopen-2012-002267
Slouma, M., Bouzid, S., Kharrat, L., Tezeghdenti, A., Ghazouani, E., Metoui, L., … Louzir, B. (2023). Ab0995 Assessment of Matrix Metalloproteinase-3 in Spondyloarthritis: Correlation With Disease Activity. Annals of the Rheumatic Diseases, 82(Suppl 1), 1718.2-1719. https://doi.org/10.1136/annrheumdis-2023-eular.5633
Sturgeon, J. A. (2014). Psychological therapies for the management of chronic pain. Psychology Research and Behavior Management, 7, 115–124. https://doi.org/10.2147/PRBM.S44762
Veehof, M. M., Oskam, M. J., Schreurs, K. M. G., & Bohlmeijer, E. T. (2011). Acceptance-based interventions for the treatment of chronic pain: A systematic review and meta-analysis. Pain, 152(3), 533–542. https://doi.org/10.1016/j.pain.2010.11.002
Wilson, N., Liu, J., Adamjee, Q., Di Giorgio, S., & Lempp, H. (2022). P250 The emotional impact of axial spondyloarthritis: a systematic review and thematic synthesis of qualitative studies and a review of online fora. Rheumatology, 61, Suppl 1, keac133.249. https://doi.org/10.1093/rheumatology/keac133.249
Zhao, P., Yoo, I., Lancey, R., & Varghese, E. (2019). Mobile applications for pain management: An app analysis for clinical usage. BMC Medical Informatics and Decision Making, 19(1), 1–10. https://doi.org/10.1186/s12911-019-0827-7
Zhao, S. S., Radner, H., Siebert, S., Duffield, S. J., Thong, D., Hughes, D. M., … Goodson, N. J. (2019). Comorbidity burden in axial spondyloarthritis: A cluster analysis. Rheumatology (United Kingdom), 58(10), 1746–1754. https://doi.org/10.1093/rheumatology/kez119
Rheumatology a New Dawn in Africa but what about Advocacy?
Author Maranda van Dam- ASIF Trustee, Chairperson ASASA South Africa
There is a massive lack of rheumatologists in Africa. According to a study done by the ACR in 2015, the ideal ration would be 2:100 000.
Africa currently has 150 rheumatologists serving a population of 1.25 billion, which is a mere 0.012:100 000. The majority of the rheumatologists (85) are in South Africa (60 million population) with the remaining 65 serving 1,240 billion people.
A roadmap must be created to increase the number of rheumatologists and enable more equitable access to healthcare across Africa.
Maranda van Dam and Prof. Olyfemi Olafipp Adelowo
In contrast to earlier reports, rheumatological conditions are now not considered to be rare in Africa and several articles reflect this. With globalisation on the increase, we are seeing migrants from Sub-Saharan Africa, living in the West, where they receive good attention and care.
The African League of Association (AFLAR) represents all 54 countries in Africa; and on 22 February I travelled to Nairobi, Kenya to attend its conference.
__________
The first day was spent doing clinical training at the AGA Khan University Centre, where topics included examination of the upper limbs, lower limbs and spine. The joint injection workshop was also highly rated by the scholars.
The keynote speaker at the AFLAR Conference was Prof Anthony Woolf, handling an important topic of the Global Burden of RMSs, and how the global rheumatology community should respond.
Herewith his key messages:Musculoskeletal health is central to wellbeing and healthy independent lives. Musculoskeletal disorders are common in all countries and cultures. In fact, the impact across Africa is much larger than previously thought.
This major cause of disability places a significant burden on health and social care. There are effective ways of preventing and controlling musculoskeletal conditions but these are not implemented with equity. There is a lack of policies and priorities for musculoskeletal conditions and investments in prevention, treatment, education and research.
Prof. Woolfs’ key recommendations were to educate and engage communities and governments, integrate MSK health into policies, build capacity, sustainable financing and surveillance. The importance of the strategic work at the WHO regarding MSK diseases could not be understated.
__________
Over the next two days we listened to revealing abstracts out of different parts of Africa, and herewith some highlights:
Nairobi, Kenya – a call was made for urgent registries for understanding the burden and impact of MSK and autoimmune diseases in Africa and improving the diagnosis, treatment and management of these diseases.
East Africa – a total of 1089 community consultations in Zambia and Kenya were completed and a total of 271 people reported with MSK issues. Only 3% represented inflammatory joint disease.
Nigeria– a total of 127 SpA patients were seen over a 12 year period, with 81% having AS. This demonstrates the prevalence of axSpA in North West Nigeria. HLA-B27 was prevalent, as was a significant delay to diagnosis.
Dakar, Senegal – 23 cases were found associated with this disease of which 76% were females. The HLA-B27 gene was found in 52% of the cases.
The key takeaways from AFLAR were:
Massive shortage of specialists care across the continent
No access to correct medications and care
Shortage of MRI imaging
Many countries in Africa do not have their own rheumatologists
No robust data available to support funding.
Development of accurate registries
No excising patient support networks in Africa for RMD’s
__________
Unlike South Africa and Algeria, patient support networks for axSpA are a foreign concept in the rest of Africa. I only found one other patient group that attended the conference (they support people with SLE). This was a topic of much discussion during AFLAR, the birth of patient support and advocacy across Africa and in all the continents that have rheumatologists. Africa not only has a shortage of specialist care for our RMD patients, but patient support is extremely uncommon.
The paucity of epidemiological data is partly driven by the low number of practicing rheumatologists in Africa.
Parts of Africa have widespread infectious diseases like HIV and hepatitis and regular breakouts of cholera, malaria and measles. Resources and medical care are funnelled to take care of these patients, RMD resources being much less prioritised.
The role of the traditional healer plays a massive role in the delay to diagnosis of a lot of patients; in South Africa 80% of the population seek health care from traditional healers and many people seek health care from both traditional and western medicine.
It is essential to invest in the development and maintenance of accurate patient registries across Africa to address the high burden of musculoskeletal and autoimmune diseases on this continent. Registries can also monitor the quality of care for patients with MSK diseases.
The importance of patient support is lost in most parts of Africa. Education, especially with a focus on West, East and North Africa, needs to be the focus over the next 5 years. It should have a special focus on the role a patient support network can have on already overburdened specialists.
During the AFLAR Conference, I presented two abstracts, on behalf of ASIF and the Axial Spondyloarthritis Association of South Africa (ASASA). I spoke about Delay in Diagnosis Spondyloarthritis, in South Africa and Understanding Mental Health in patients with Axspa. The abstracts were received with much enthusiasm and many questions. Hearing from a patient group was indeed a foreign occurrence for most in the room.
As a new dawn breaks in Africa for rheumatological diseases, a massive need for patient advocacy and support groups will grow exponentially. The lower income countries rely heavily of Western countries for support and education, which makes this hopeless situation seem less so. Most of the African countries now require their specialists to qualify with the EULAR educational course, which sets the bar for the training very high.
There is no doubt that the growing number of RMD patients across Africa will create a massive burden on patient care and support systems. The role of patient support is a crucial element of a normal health system. The needs of a RMD patient are often much more than a clinical appointment. In the foreseeable future Africa will face the challenge of offering patient support to already impoverished countries.
As one of our colleagues said during the conference: ”If you do not think that you will make a difference, no matter how small you are, you have clearly not been in a room with a mosquito”.
REFERENCES:
Ibrahim DA, Na’Isa MBK, Hamidu A, Profile of Spondyloarthropathy patients in Kano, Northwestern Nigeria, African Journal of Rheumatology Volume 11, January 2023m ISSN 2307-2482
Charifah S, Niasse M, Gueye YA, Diallo S, Spondyloarthritis and autoimmune diseases: preliminary study of 23 Senegal Cases
Genga EK, Call for Action: development of patient registries in Africa
It was with great sadness that we learned of the passing of Prof. Dr. Ernst Feldtkeller at 92 years of age (October 19, 1931 — January 4, 2023). He was truly a remarkable and inspiring person, scientist, and researcher, with a PhD in Physics. He was appointed Professor at the Universities of Stüttgart and Munich, and a researcher at the Siemens Research Laboratories in Munich. He had suffered all his adult life from ankylosing spondylitis (frequently called Morbus Bechterew in German-speaking countries), and in 1980 he played a pivotal role in the formation and subsequent management of the German Ankylosing Spondylitis Society named Deutsche Vereinigung Morbus Bechterew (DVMB).
Prof. Dr. Ernst Feldtkeller
He authored an excellent book in German on ankylosing spondylitis for educating patients and their families and was the Scientific Director of the editorial office of the DVMB membership journal called Bechterew Brief. He was fluent in English, and he used to translate important English publications into German for the readers of his Journal. He selflessly put all his creativity, knowledge, and skills into the service of the DVMB and other organisations over the last 42 years.
On 8 April 1988, Ernst became a member of a committee that was formed, at the invitation of Fergus Rogers (of National Ankylosing Spondylitis Society, U.K.), to carry out the preliminary preparations necessary for the foundation of an International Ankylosing Spondylitis Association (which later became Axial Spondyloarthritis International Federation – ASIF). He was invited to attend the first ASIF Council Meeting in Leukerbad, Switzerland in July 1989, hosted by another remarkable patient and scientist Dr. Heinz Baumberger, PhD [1]. He was elected as a Vice-President of ASIF in 1992, a position he held until 2009. Thereafter, he served as ASIF’s Scientific Adviser until retiring from this role in 2017.
After his retirement from Professorship in 1992, Ernst devoted his full attention to doing scientific studies and clinical research in ankylosing spondylitis. In 1996 he obtained financial support from the German Federal Health Ministry and initiated a professional survey among the more than 14,000 patient members of SVMB. 1614 patients responded to this survey, and extended reports of the results were published in five issues of Bechterew Brief in 1997-1998. He then presented these results in English at the 1st International Congress on Spondyloarthropathies, in September 1998 in Gent, Belgium. Over the years Ernst had published many highly cited articles in German and English, and based on his extensive contributions, he was awarded membership of the Assessment of SpondyloAarthritis international Society (ASAS).
Ken Mulholland (ASIF Secretary 2002-2011) recalls meeting Ernst at the first ASIF Council Meeting; “My early impression of Ernst was his extensive knowledge of the disease, his research, and his extensive publications. Over the years, I got to know Ernst little more and see how instrumental he was in introducing Ankylosing Spondylitis to the world through his development of the ASIF website. Ernst was very meticulous in all his workings.”
I first met Ernst at the first ASIF Council Meeting in Leukerbad in 1989 and we became lifelong friends and co-authored two of his many highly cited publications [2, 3]. I frequently exchanged with him articles of interest and helped maintain Ernst’s remarkable personal library of articles from medical journals stored either digitally in a PDF format or, in some cases, as printed documents. He shared his personal library with me, and I sincerely hope that it will be kept alive and up to date.
Ernst’s other interests extended to mountaineering, cycling, playing the flute, and painting beautiful watercolour landscapes (pictured), many of which he generously gave away to friends and colleagues. He was also an avid photographer, always carrying his camera with him, and he regularly summarised important scientific meetings along with pictures of scientific presenters.
With Prof. Dr. Ernst Feldtkeller we have lost a valued companion, a respected fellow patient, and a good-hearted and charismatic personality. His unparalleled commitment, diligence, frugality, and modesty were an example to us all.
With his exemplary commitment to those affected, Ernst Feldtkeller earned a high and lasting reputation in the global spondyloarthritis community. Ernst’s contributions to DVMB and ASIF, and to the rheumatology and patient communities at large, will be sorely missed.
REFERENCES:
Khan MA., Accomplishments of Heinz Baumberger PhD: A remarkable patient with ankylosing spondylitis for 72 years, Clin Rheumatol. 2016 Jun;35(6):1637-1641. doi: 10.1007/s10067-016-3259-0.
Feldtkeller E, Bruckel J, Khan, MA., Scientific contributions of ankylosing spondylitis patient advocacy groups. Current Opin Rheumatol. 2002 Jul;12(4):239-247. doi: 10.1097/00002281-200007000-00002.
Feldtkeller E, Khan MA, van der Heijde D, van der Linden S, Braun J., Age at disease onset and diagnosis delay in HLA-B27 negative vs. positive patients with ankylosing spondylitis, Rheumatol Int. 2003 Mar;23(2):61-66. doi: 10.1007/s00296-002-0237-4.